
Welcome to Orthosports Question for Physiotherapists May 2025. This month Dr Leigh Golding discusses internal impingement of the shoulder.
REMINDER: SAVE THE DATE Orthosports Annual Orthopaedic Updates, Saturday, 8th November, 2025, live @UNSW or via webinar. Registrations open later in the year.
If you have a Question that you would like answered on this monthly email please send to education@orthosports.com.au

QUESTION | A 25‐year‐old male baseball pitcher presents with posterior shoulder pain during the late cocking phase of his delivery. He reports morning stiffness, a decrease in pitch velocity, and pain that is reproduced on resisted internal rotation. How would you approach managing this?
Internal impingement is common among overhead athletes, and particularly common in throwing sports such as baseball and cricket. It occurs when the greater tuberosity of the humerus impinges against the posterosuperior glenoid rim during positions of abduction and external rotation, leading to compression of the articular surface of the rotator cuff. Adaptive changes—such as posterior capsular contracture and scapular dyskinesis—often contribute to this pathology [1].
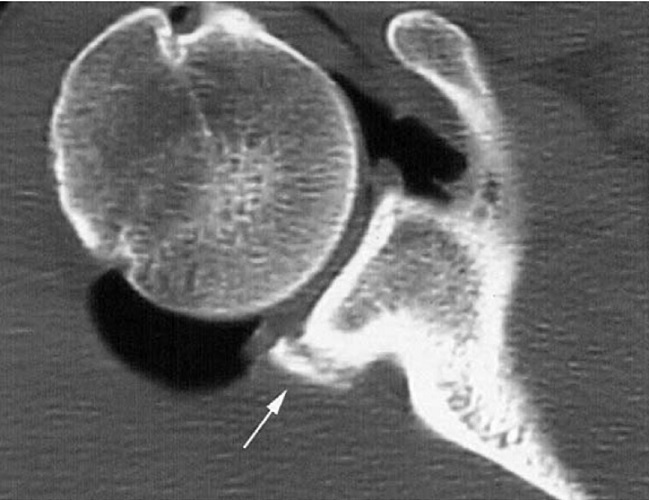
The clinical examination typically reveals reduced internal rotation on the affected side compared to the non‐throwing shoulder. In addition to observing scapular dyskinesis and measuring range-of-motion deficits, several diagnostic tests can help confirm the diagnosis. For example, the posterior impingement test (performed with the arm abducted 90–110° and maximally externally rotated) frequently reproduces the patient’s pain. The relocation test, resisted internal rotation, and apprehension tests are also useful diagnostic maneuvers, while palpation may reveal tenderness along the posterior glenohumeral joint. Plain X-rays may show a Bennett lesion. MRI can clarify diagnostic uncertainty, often revealing associated articular-sided partial-thickness rotator cuff tears or SLAP lesions [2].

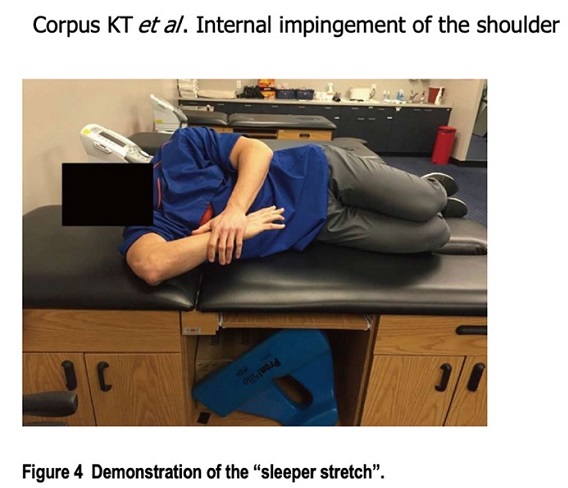
Management begins with offloading the shoulder by modifying or temporarily avoiding provocative activities (e.g. throwing). In the initial phase, conservative treatment focuses on pain control—using anti-inflammatory modalities—and gentle range-of-motion exercises. Stretching techniques, such as the “sleeper stretch,” are employed to alleviate posterior capsular tightness and improve internal rotation. Although corticosteroid injections may be used diagnostically in some instances to confirm the pain source, they are generally avoided as a long-term therapeutic option.
Rehabilitation should progress in a structured, phase-based manner. Early-phase rehabilitation emphasizes restoring range of motion and scapular stability through controlled stretching and neuromuscular re-education exercises. As pain subsides, a progressive strengthening program is introduced to rebalance the shoulder musculature. It is critical to target both the internal and external rotators; in healthy throwers, the external rotators should generate at least 66–75% of the force produced by the internal rotators [3]. Specific strengthening exercises include isometric contractions progressing to dynamic resistance exercises (both concentric and eccentric) for the external rotators, which are essential for decelerating the arm during throwing.
Finally, a gradual, supervised return-to-play (return to throwing) protocol is crucial. The athlete should progress from controlled therapeutic exercises to sport-specific drills, ensuring that sufficient strength, range of motion, and neuromuscular control are restored before resuming full competition. In throwing athletes, throwing load and intensity should be titrated carefully as symptoms allow.
Internal impingement can significantly compromise throwing performance, making early diagnosis and intervention critical. Without prompt management, athletes risk prolonged rehabilitation and extended time away from their sport. Collaborating with experienced practitioners in the diagnosis and treatment of internal impingement can help facilitate a timely return to play.
In cases that are refractory to high quality conservative care, arthroscopic surgical intervention, typically involving excision of the Bennett lesion, posterior capsular release, and debridement or repair of SLAP tears or partial-thickness rotator cuff tears may be necessary to enable optimal recovery and return to performance.
References
[1] Corpus KT, Camp CL, Dines DM, Altchek DW, Dines JS. Evaluation and treatment of internal impingement of the shoulder in overhead athletes. World J Orthop. 2016;7(12):776-784.
[2] Nakagawa S, Yoneda M, Hayashida K, Mizuno N, Yamada S. Posterior shoulder pain in throwing athletes with a Bennett lesion: Factors that influence throwing pain. J Shoulder Elbow Surg. 2006;15(1):72-77. https://doi.org/10.1016/j.jse.2005.05.010
[3] Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30(1):136-151.