
Welcome to Question for Physiotherapists April 2026. This month Dr Paul Annett discusses localised buttock pain and proximal hamstring tendonopathy.
Save the Date: Saturday, 1st August 2026 for the 2026 Orthopaedic Update at UNSW and via webinar, invitations coming soon!
If you have a Question that you would like us to answer or have a colleague that would like to be included on our mailing list please email: education@orthosports.com.au
On history the patient generally has well localized pain to the ischial tuberosity, and this is typically worsened by periods of prolonged sitting, especially on hard surfaces and particularly when driving. It is more likely to cause symptoms with walking up hills and stairs rather than on the flat, and running is typically the most provocative activity.
Examination findings may include pain on lumbar flexion. Double or single pelvic bridging may provoke pain, as may resisted knee flexion (hamstring curl), with associated weakness. Direct palpation to the ischial tuberosity may cause tenderness, but the degree can be underwhelming. Examination also needs to exclude other potential causes of buttock pain, including lumbar radiculopathy, sacroillitis or hip joint pathology.
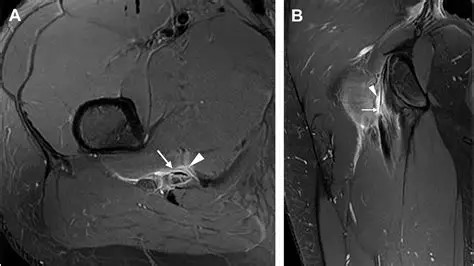
Imaging may include plain Xray, ultrasound or MRI. Xray is a useful test to assess for degenerative hip or sacroiliac disease, pelvic stress fracture or unexpected nasty pathology. Ultrasound can demonstrate thickening or calcification of the proximal hamstring tendon, but does lack accuracy when compared to MRI. MRI is much better at demonstrating tendonopathy with associated partial tearing. It can also assess for other soft tissue abnormalities such as ischiofemoral impingement. The scan will also address possible bone or joint pathology such as a sacral or pelvic stress fracture or hip or SIJ degenerative change.
The management of proximal hamstring tendonopathy is similar to that of other tendinopathic conditions. Confirmation of diagnosis is an essential first step, whether that be from textbook clinical findings or with supportive imaging. A period of unloading is essential. This is typically an issue in runners where load needs to be reduced. This may include reduced volume, intensity and avoiding stressors such as hills and stairs. Appropriate manual therapy needs to be commenced around the hamstring, buttock and lumbar spine. Rehabilitation exercises should also be started and graded from isometric to eccentric and concentric hamstring strengthening and addressing any gluteal weakness and loss of pelvic stability.
Interventional therapy is generally injection based including both cortisone or PRP. Cortisone may be indicated in cases with more acute inflammation, such as ischial bursitis or peri-tendinitis, where the structure of the tendon is still maintained. In cases of more significant tendonopathy, especially including partial or intra-substance tears, then PRP is a preferred alternative. Whilst there are limited studies regarding this, one suggested 68% of patients improved by more than a 50% reduction in pain after a single injection(1). Surgery is typically not indicated unless there is a complete disruption of the tendon attachment or protracted symptoms resistant to other appropriate treatment modalities.

Reference:
1. Platelet-rich plasma for treatment of chronic proximal hamstring tendinopathy, April 2020, Regen Med