
Welcome to Orthosports Question for Physiotherapists July 2024. This month Dr Paul Annett discusses Tarsal coalition.
REMINDER: SAVE THE DATE Orthosports Annual Orthopaedic Updates, Saturday, 9th November 2024, live @UNSW or via webinar. Registration opens in August.
If you have a Question that you would like answered on this monthly email please send to education@orthosports.com.au
QUESTION | I have recently sent a patient for an MRI scan for ankle pain, and they were diagnosed with a tarsal coalition. Could you explain this condition and how it should be treated?
A tarsal coalition is a condition where there is an abnormal connection between 2 or more bones in the foot. Tarsal coalition occurs between 1-13% of the population. The precise incidence may be hard to determine as many will remain asymptomatic. Tarsal coalition is a failure of normal mesenchymal segmentation in the foot. The 2 most common sites are between the talus and calcaneus (talocalcaneal coalition) and the talus and navicular (talonavicular coalition). These 2 sites are of equal incidence. In approximately 50% of cases both feet are affected. The abnormal connections are known as ‘bars’, and may be made of bone, cartilage, or fibrous tissue. The coalitions are present at birth but are generally not symptomatic until early adolescence.
Presentation
As mentioned previously many coalitions are asymptomatic and are never discovered. Symptoms when they occur may include stiffness or pain, predominantly in the rearfoot. There may be rigidity with a flat foot that can make it difficult to walk on uneven surfaces. Another presentation is the development of recurrent ankle sprains due to reduced sub-talar joint motion. Presentation typically occurs in adolescence, with calcaneonavicular coalition presenting earlier and talocalcaneal presenting in later adolescence.
Examination findings
The classic finding in a tarsal coalition is rigid everted rearfoot with associated peroneal spasm. When the patient is asked to stand on their toes they will lose the normal heel inversion. There will be significant loss of rearfoot motion and sub-talar joint stiffness.


Imaging
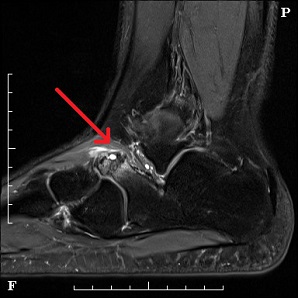
In some patients’ plain x-ray will demonstrate the coalition if there are changes of a bony bar. Classic X-ray findings are of the ‘anteater nose’ of the talonavicular coalition, and the ‘C sign’ of the talocalcaneal coalition. Whilst CT scan may be more accurate for bony changes an MRI is the most accurate way of detecting soft-tissue and cartilage coalitions and also demonstrating reactive bone marrow oedema which may suggest activity of the coalition.

Treatment
Tarsal coalitions only need treatment if they are causing symptoms. Treatment may be non-operative and operative.
Non- operative treatment may include:
Rest – Simply avoiding sport for 4-6 weeks can reduce stress on the tarsal bones and relieve pain.
Immobilization – Boot or cast immobilization for 6 weeks can relieve pain.
Orthotics – Improved foot mechanics may relieve pain.
Cortisone injections – Injections around the coalition and sub-talar joint can relieve pain.
At least a 3-month trial of non-operative therapy is appropriate before consideration of surgery. Approximately 30% of patients will improve with non-operative therapy.
Operative treatment will depend on the size and location of the coalition and whether the patient has developed secondary degenerative change.
Open resection of the coalition is the most common surgical treatment with a possible soft tissue interposition. This is generally the treatment for talonavicular coalitions, both in adolescents and adults. Resection can be performed in talocalcaneal coalitions without advanced arthrosis, hindfoot deformities or more than 50% of the joint involved. The outcome of resection for talocalcaneal coalition is less reliable than for calcaneonavicular, where fusion may be a more reliable treatment. It has been reported that the resection may be performed arthroscopically. A recent review of the literature suggested low recurrence and complication rates (1)
Fusion may be required for larger more severe coalitions with deformity, or if there has been the development of osteoarthritis in the affected or surrounding joints.
In summary, tarsal coalition is an uncommon condition which should be considered in patients with non-specific rearfoot pain and stiffness. The diagnosis can be made on accurate clinical assessment and confirmed with appropriate imaging, usually including an MRI scan. Whilst many patients will improve with non-operative therapy, when this fails effective surgical alternatives are available.
- Tarsal coalition : Systemic review of arthroscopic management. The Foot, Dec 2021