I use a 10 ml syringe with a 23 gauge needle attached. I generally use 2 ampules of Celestone Chronodose combined with 8 mls of 1% Xylocaine. A lower dose of corticosteroid is recommended for diabetics and they must be warned to monitor their blood sugar levels for up to 72 hours.
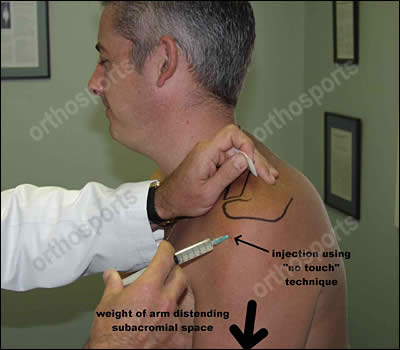
Infection can be a problem and a “no touch” technique can be used using an alcohol wipe or Betadine. If you do not have experience with a “no touch” technique then we recommend that you wear sterile gloves and use a prep tray.
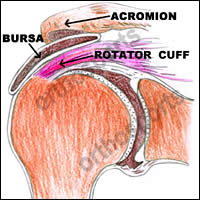
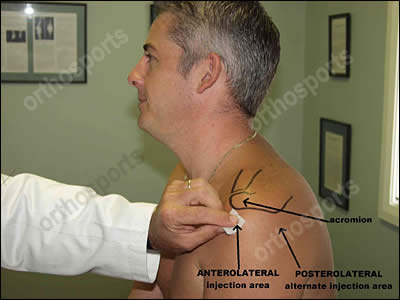
The aim of the injection is to place it under the acromion and above the rotator cuff, into the bursal area. This is a fairly large area and to make it easier to access, I have the patient sitting upright, so the weight of the arm opens the subacromial space even wider. I approach the subacromial space from an anterolateral direction. Many doctors find the posterolateral direction more to their liking and it is up to each doctor to use the approach with which they feel most comfortable. Once the needle is in position push the plunger of the syringe. The fluid should enter the subacromial space with ease. If there is any resistance stop, reposition the needle and inject again.

Given correctly this injection is rarely painful but the patient may get some rebound pain after 2 hours when the local anaesthetic wears off.
With any procedure there are risks and complications. These include but are not limited to infection, allergic reactions and severe pain. All of these are exceedingly rare. It should be noted that diabetics may get a transient rise in their BSL.