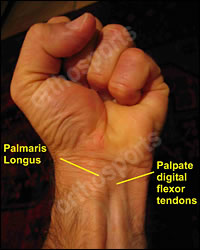
Palpate digital flexor tendons as the fingers flex and extend.
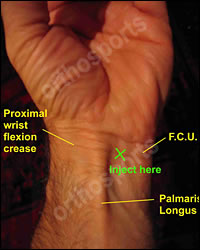
The Median nerve is radial to Palmaris longus, between this tendon and the FCR tendon.
Use of Carpal Tunnel Injections
A good response to a cortisone injection can:
Help differentiate between Compressive neuropathy, e.g. CTS and other types of neuropathy, e.g. Diabetic.
Help differentiate between Carpal tunnel syndrome and Cervical spondylosis and the degree to which each condition contributes to a particular patients symptoms in a double crush syndrome.
Act as a positive prognostic indicator for a good subsequent response to a carpal tunnel decompression. If a patient does not improve with an injection I would be very reluctant to recommend surgery.
Carpal tunnel injection is not a useful test unless a clear end point can be identified.
i.e. complete resolution of symptoms, ability to sleep.
in severe cases of late CTS when numbness is constant and patients may not still be waking from sleep, injection of cortisone is not a useful test.
Technique
1 ml Celestone + 1 ml Lignocaine.
Mark entry site with finger nail.
Clean with alcohol swab then no touch technique.
Pass needle through skin quickly with the needle bevel parallel with nerve and then inject a small amount of fluid just under the skin.
Wait 20 – 30 seconds then gently advance the needle while getting the patient to gently flex and extend their fingers.
Continue injecting. If fluid bulges the skin and fat it is superficial to the deep fascia. ie too superficial. When the flexor tendons can be felt moving against the end of the needle the needle is deep enough.
If the needle moves with finger ROM it is in the tendon!!! and should be moved.
Inject slowly and not against resistance. It should be painless. If you elicit paraesthesiae stop and reposition the needle.
Ask patient to note what benefits are obtained over the next few weeks.